Check In and Report Out
John Becher
Good morning to our final day of the summit. And in our continuing tradition, here is our daily poem.
 Did I Miss Anything
Did I Miss Anything
Question frequently asked by
students after missing a class
Nothing. When we realized you weren't here
we sat with our hands folded on our desks
in silence, for the full two hours
Everything. I gave an exam worth
40 per cent of the grade for this term
and assigned some reading due today
on which I'm about to hand out a quiz
worth 50 per cent
Nothing. None of the content of this course
has value or meaning
Take as many days off as you like:
any activities we undertake as a class
I assure you will not matter either to you or me
and are without purpose
Everything. A few minutes after we began last time
a shaft of light descended and an angel
or other heavenly being appeared
and revealed to us what each woman or man must do
to attain divine wisdom in this life and
the hereafter
This is the last time the class will meet
before we disperse to bring this good news to all people
on earth
Nothing. When you are not present
how could something significant occur?
Everything. Contained in this classroom
is a microcosm of human existence
assembled for you to query and examine and ponder
This is not the only place such an opportunity has been
gathered
but it was one place
And you weren't here
There's an article in today's paper. Down with dead doctors.
Yeah, down further. (laughter)

Report Out of Last Round of Work
GMP - Shifting Paradigm Summary
http://nationalalliance.pbwiki.com/GMP1:+Shifting+Paradigm+Summary
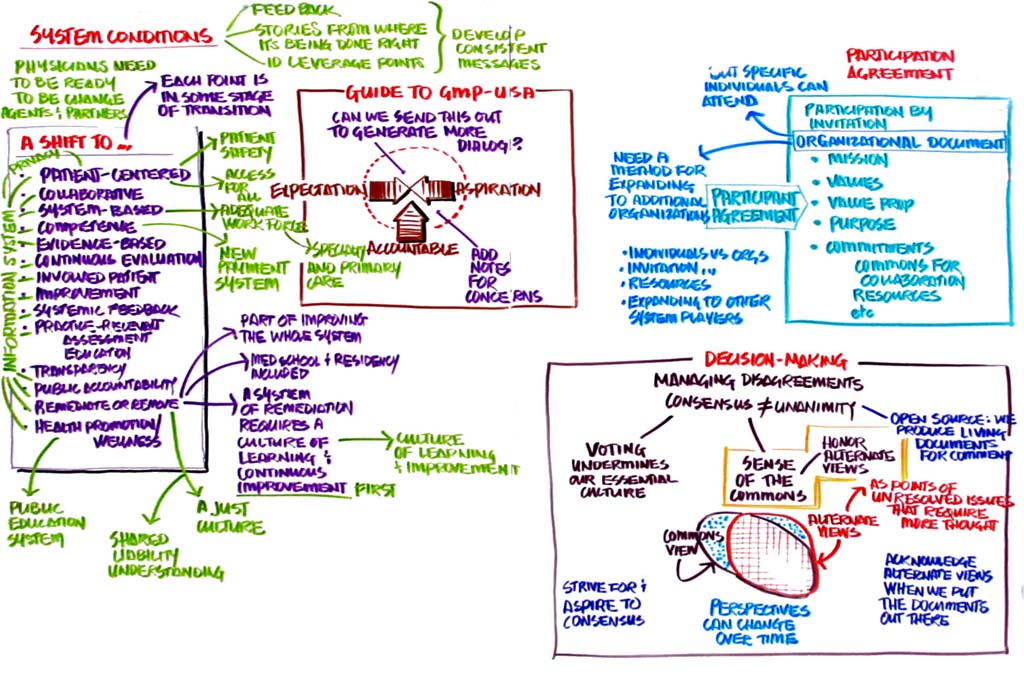
 From an idiosyncratic system, we want to have a knowledge based-system and have a evidence-based standards. Most of our system has been anecdotal. We want to move from a system that goes from opaque to transparent. We ignore the questionable competence of people and now we address these issues.
From an idiosyncratic system, we want to have a knowledge based-system and have a evidence-based standards. Most of our system has been anecdotal. We want to move from a system that goes from opaque to transparent. We ignore the questionable competence of people and now we address these issues.
On the white boards, we also ranked where we are in the transition for each of these areas. These are new ideas for us but when you put everything together in one place, it becomes quite a story.
Q: Was there anything unique or different from any of the other group's posters that should be considered on its own?
A: I suspect there were and we needed more time to address that. That would be a good exercise to do.
Q: Have you focused on questionable competence and remediation in any of these conversations?
A: I think we have. Two summits ago when we were looking at different systems, we looked at re-entry and remediation and what the new system would look like. We talked a lot about the admissions process and making decisions earlier on who should or should not be a physician.
There was also an acknowledgement that we had a code of not ratting on our colleagues and we addressed needing to change that. Maybe we need to laser in on the ones who have real issues?
In the U.S. there is no system of remediation. Some of them would be better off with the dead doctors (laughter). There is no system of training for doctors that need to improve. It’s something that needs to be done but this is also part of the culture change.
The word ‘remediate’ may not be the right one if you have a culture of learning.
The shift group came up with the first 12 items here, the last two were added by people who came to visit our group.
I think we need to have more non-physicians embedded in our system and in our discussions. Yes, this is more difficult than peer review, but I think its essential.
MK: There is a movement and a shift taking place. These may be the elements of what’s taking place. Is there anything you can’t live with in this list?
No.
These are not ‘either/or’ but sometimes a continuum.
Alliance Participant Agreement
http://nationalalliance.pbwiki.com/na1:++Alliance+Particpant+Agreement+Review
 It was good to have new colleagues in this place. This has a list of commitments. We’re looking at voluntary and invitational participation.
It was good to have new colleagues in this place. This has a list of commitments. We’re looking at voluntary and invitational participation.
Comment: I struggle with the notion of your language. Our history hasn’t been to extend invitations, but are open to anyone who expresses an interest in coming.
That language was carried over from the previous document. We kept it in because we could imagine a time when there is an organization that the rest of the participants might not want to include.
In the last summit we talked about the malpractice attorneys union wanting to join, but we’re not sure that we’d want to have them.
Unless we incorporate or pass by-laws, we’re spending too much time on this document. This is informal. I think this document is really good. No one has been turned away yet. It’s not that we would deprive individuals from coming but having people who have a substantial impact of what we’re doing can come. I would support this document as they have written it.
We could look at who’s involved in making the decisions. We did come up with a model as well as skill-sets necessary and in order to move this forward we want organizations which contribute financially and in-kind support.
We should take another look at this.
How do we make decisions?
http://nationalalliance.pbwiki.com/na4:++How+do+we+make+decisions
 We recognize that there are difficult conversations that we have to have. In dealing with a particular process that’s involved, we must reach unanimity. So we suggest calling on the voice of the commons for making decisions. We don't want to vote as we haven’t worked out exactly how votes might count. In addition to the voice of the commons we have to find a way to acknowledge and record alternative views.
We recognize that there are difficult conversations that we have to have. In dealing with a particular process that’s involved, we must reach unanimity. So we suggest calling on the voice of the commons for making decisions. We don't want to vote as we haven’t worked out exactly how votes might count. In addition to the voice of the commons we have to find a way to acknowledge and record alternative views.
The way the two circles are shown in this diagram suggests we need to find a way to encompass the overlap more than we have in the past.
There is something about it that seems to support the least common denominator. We want to find where the alternative views makes the whole thing better.
We don’t want to accommodate or please everyone - which is impossible. The concern is that this group has come a long way. The concept of being leaders here we need to find ways to move ahead even if we don’t have unanimity.
The only thing the alliance does is produce documents for comments. It doesn’t make any decisions. If there are disagreements, we need to have a path for dealing with that. We can document the disagreements and people can see them.
This is viewed as a living document. There were suggestions for incorporating feedback. Consensus is good, but we don’t want the majority to be held hostage by the minority.
As long as we incorporate the alternative views so that they are part of the record and don’t disappear. Circumstances and perspectives will change.
It would be good to formulate the alternative views so that they become points of discussion and inquiry.


GMP
http://nationalalliance.pbwiki.com/na9:++GMP+Document
 We decided to change the name to the Guide to Good Medical Practice.
We decided to change the name to the Guide to Good Medical Practice.
The panel originally decided to use the term doctor to be more inclusive because for example I have a license for being both a physician and a surgeon. We’re not talking about doctors of pharmacy or dentistry or nursing, but we didn’t want to separate the doctors of specialties. We can change it to physician.
We could say privileging or credentialing in order to incorporate the specialties.
There might be a need to use the word physician consistently given that this is the alliance for physician competence.
We want to be clear about this being aspirational as opposed to being goal-oriented.
The document describes desirable characteristics. I think the word aspirational waters it down. (Almost everyone agrees). Okay, we take aspirational out and make a side note that some people would like it in.
We’ve already called it a guide so it points to something like that.
I don’t care if we use the word or not. We need to point out that these are ideals that we aspire to as a physician. You can still be a competent physician without meeting all of these qualities.
I disagree. The public is not that unreasonable. I think we can argue about what substantial means. If we start picking this thing apart because you’re afraid of liability, you’ll destroy it.
We’ve tried to find language that expresses the fact that not all doctors can do all of this all the time. No doctor is going to be thrown in the trashcan if they don’t meet all of these qualities all the time. I would be disappointed if we need another two summits to get to this document. Maybe we need some more dialogue about firmer words about qualities and expectations? I hear we should go further this way or that. Have we reached a ground where it is good enough for now?
There are not a lot of practicing doctors in this room. Where does it tell them that if they don’t do these things, that they’re incompetent?
Being held accountable doesn’t mean you’re all of this all the time. I think if we put in ‘ideal’ or ‘aspirational’ then it sends the message that we’re not ready for this.
We need to gather feedback on this. Not to push it out to people that think they will be held accountable based on this, but is it good enough to send out to find out its potential utility?
We need to acknowledge that there are rationales behind the different opinions. We can still keep people under one group and have columns which voice the concerns, so any legislators can see that.
Does failure to achieve one of these necessarily mean you can be punished? We could put something in there about that.
I think if we tinker with minimizing the impact of this document, what is the point of it?
I think we add, "a doctor will “strive” to achieve these things."
I don’t think that it implies either you’re competent if you meet all the bullets or incompetent if you don’t. It only points to what can be improved.
This is a really valuable document and we don’t want to have knee-jerk responses when we put it out. Some of the tension here is to get it into a form that will be accepted by a broad group of people.
We’re looking at something to send out that all physicians will see. All physicians now have a way of guidance that we can see. It’s easy to say you’re God and have only your own internal qualifications. This way we can provide something that all can see.
I’ve seen in two summits so much work. I think we should frame this openly. Many don’t realize how wounded this profession is. We have a psychology of victimization that we have to attend to.
If we were to look at the bottom of this document, you would see that there is no way that we could get through this entire thing in this session. We could identify the subset of items that have a lack of consensus. We can’t allow that process to inhibit the rest of the document and its dissemination. We didn’t ‘want to tinker with the 225 examples. We’re aware that there is an effort of gathering a broader set of input on those.
We did make a significant change around the respect of the patient’s time in terms of making it broader instead of limiting it to just being on time for appointments.
I make a request for a sense of the commons. It is good enough for the dissemination for other comments?
Hear hear! (No one disagrees.)
I have a request to have clarity around the wording of doctor versus physician. Can we say that this applies to doctors of medicine and osteopathy?
A sense of the commons? Physicians.
Q: Is this a time-limited vetting process?
A: We didn’t address that.
The conditions for GMP
http://nationalalliance.pbwiki.com/na8:+System+Conditions+to+Enable+GMP
 We looked at what the system has to be so we can do what we want. The frame for this is that this is a first rough pass at what we would envision as another appendix to the GMP document. We need to have physicians who are willing to lead system change. This means having a vision, voice and influence, as well as learning new skills.
We looked at what the system has to be so we can do what we want. The frame for this is that this is a first rough pass at what we would envision as another appendix to the GMP document. We need to have physicians who are willing to lead system change. This means having a vision, voice and influence, as well as learning new skills.
We need an information system, not necessarily electronic though that would help, so we can assess performance and patient outcomes in order to assess competence. I’m sure there are others of you out there who can put better words to this.
We got the idea from our Minnesota colleagues of a just culture, correcting errors rather than blaming people. We want to educate organizations and individuals about system errors and to discipline only if the error is intentional.
Q: How do you know if it’s intentional?
A: That’s a great question and maybe we can find out more from our Minnesota colleagues about that.
It’s not that we would wait for all these conditions to be in place to be a competent doctor. We want the remuneration as a way to acknowledge physicians who meet the competency qualities.
We want lawmakers and policy makers to be informed of these things.
A critical system condition is that we need to be a culture of learning. We need a professional view of what a doctor really does. Part of what we can influence is the focus on what gets rewarded and counteract our current blaming culture.
We took some initial steps in getting feedback. We should identify opportunities for early advancement.
We want to take this, have a small group refine it on the wiki and then at some point have it become an appendix to the GMP document.
We have to be partners with many stakeholders and not be passive bystanders. We don’t want to say to them to get out of the way but to ask them to lead and partner with others.
I’d like to add that we should aspire to create a balance between primary care and sub-specialty specialization. We should put something about having an adequate care workforce.
This is a grand experiment. Looking at a series of reports about healthcare never once is it mentioned about the quality of healthcare in the U.S. We should take the opportunity to reach out and take this material back to the legislators. We could have the nucleus of a radically transformed healthcare system based on what you’re doing here.
Primary care has become the poor stepchild to the specializations and sub-specializations. We need to address that.
Knowing that there are problems with the system is not new. The idea of physicians contributing to the solutions is unique.
We’ll continue to work on this.
This is inimical to how we aspire to practice. This needs to address the things that are in the way of good doctors.


Dissemination of GMP
http://nationalalliance.pbwiki.com/na10:++GMP-USA+Dissemination
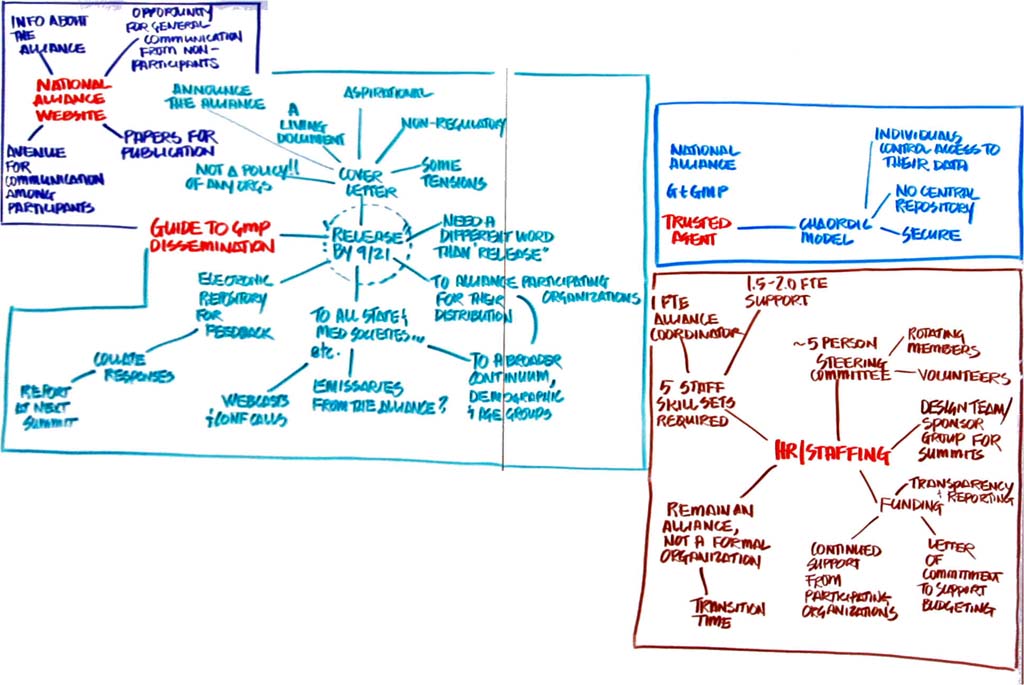
 We want to draft a letter signed by all the participants that acknowledges this is a living document and we acknowledge the contentions that we’ve discussed here. We want to distribute GMP to the stakeholders represented here at the summit and the organizations can decide how to distribute it to their constituencies.
We want to draft a letter signed by all the participants that acknowledges this is a living document and we acknowledge the contentions that we’ve discussed here. We want to distribute GMP to the stakeholders represented here at the summit and the organizations can decide how to distribute it to their constituencies.
We want to have an electronic repository of comments that are trackable, not just inflammatory missives, but with those responsible for the comments listed. Perhaps we can create a subgroup who can collate these comments and share them at the next summit? We should decide if we want further dissemination beyond the participants in the summits.
Q: Why don’t we have it labeled as 1.0?
A: Because we recognize that this is not the real final document, but the first drafts.
Q: I wonder if we can go to each state association? It would be nice to have someone from the Alliance to talk to each of them to get their feedback to incorporate in the document.
A: That kind of thing takes an organizational structure to pull off.
A: We could organize a series of webcasts to have interactive engagements which might be better than only sending it out in a one-dimensional way asking for feedback.
Someone yesterday mentioned that there isn’t much representation from the future of medicine and I think we should make a special effort to include the students and residents as they are the people who will (hopefully) live with this document more than we will.
We also need to get it to other ethnic groups that are not represented here.
Please put enough verbiage in the cover letter that this doesn’t speak to policy.
Maybe we should push back the date of release?
There are hundreds of people we have to get emails and addresses for. If we target September 21st, I don’t know if that will be when everything is already sent out. I imagine we won’t release it all the way until after the AMA meeting anyway.
This is a stimulus document not for policy. I would avoid words like ‘release’.
Q: Are we going to place a date for the feedback? It might be good to have an end.
A: We’d like to have the feedback by the next summit.
Maybe that’s what we can say. There’s no arbitrary deadline, but that we will incorporate the comments for the next iteration by the next summit.
We will be clear that we’re putting this out as a living document.
Q: Is there a sense of inviting people to the website?
A: We didn’t get into that. What we’d like to do is have a common mailbox where they can make comments.
Q: Is this also an opportunity to get more visibility for the Alliance? We may want to think about that?
A: That’s a good idea.
National Alliance Website
http://nationalalliance.pbwiki.com/na3:+National+Alliance+website
http://www.innovationlabs.com/nationalalliance/index.html
 The idea is to have a web site for the Alliance and to move what we have now off of innovationlabs.com. One of the things we talked about is that we want it to provide a forum for communication and a way to disseminate information to the world at large and find a way for them to respond to it. We considered a private log-in area.
The idea is to have a web site for the Alliance and to move what we have now off of innovationlabs.com. One of the things we talked about is that we want it to provide a forum for communication and a way to disseminate information to the world at large and find a way for them to respond to it. We considered a private log-in area.
Maybe we could have a commons area where we could have a dialogue or blog attached to the site.
This would have all the information from the summits so people could have a context of the work that has gone on here.
When we think about what it is going to take to make the kind of shift we are talkinga bout and how the Alliance will be involved in making this shift happen - that seems to be an article that is in the making. This is also a way to announce the organization among readership as it would go to a well-read specialty journal. The shift work is really powerful stuff. This is the group that can say that this is the shift we need.
Trust Agent
http://nationalalliance.pbwiki.com/na5:++eFolio+Framework
 The trusted agent is the mechanism for sharing information. We’re trying to develop a way to access data from one point and serve as a conduit to another point. We can use this kind of thing for self-assessment. We need to develop an IT capability that is not central so that the physicians can control their own portfolio. We’re still working on the logistics for how to make something like this happen.
The trusted agent is the mechanism for sharing information. We’re trying to develop a way to access data from one point and serve as a conduit to another point. We can use this kind of thing for self-assessment. We need to develop an IT capability that is not central so that the physicians can control their own portfolio. We’re still working on the logistics for how to make something like this happen.
Norm Kahn - IPIP: Improving Performance in Practice
 And now for something completely different.
And now for something completely different.
We’ve been talking about aspirations and planning for a desired future, but now we’re going to talk about reality. I want to do this in a way that will feel real because it is real. I want you think about the shift document.
This map of the U.S. will show you the reality. Over here is Philadelphia, there was a vision to look at maintenance of certification and find a way to show improvement in nationally accepted measures for chronic illnesses. We created Improving Performance in Practice.
The Robert Wood Johnson Foundation has funded this at a national level. In Chicago the decision was made that the infrastructure support would be housed at AMIS. This was supposed to be a project identified with specialty societies and not certifying boards. Shelley Horowitz is the principle investigator. At this point in time there are 7 states which are participating.
We’re going to focus on Colorado and North Carolina which were the only two states until spring of this year. Thirty practices were enrolled. These are the innovators and early adopters. If you could hone down on various practices and put yourself in that practice for a moment. What do you need? You don’t need an electronic health record. Fourteen of the practices had this but not a registry. It’s a distraction because there is so much that is necessary. It’s better to have a registry.
We can take diabetes and asthma because there are clearly idenitified symptoms and treatments. You can put in a patient registry and then you need someone who can coach these practices. They’re going to meet every other month. They’re going to be quality improvement coaches. You have to give them data based feedback. The data goes to the University of NC and Children’s Hospital of Cincinnati. Originally there were 24 nationally accepted measures but that’s too much. We took just a few: blood pressure, LDLS, hemoglobin A1C, eye exam, nethropathy, and smoking stats. As a quick aside, there is a tool called Archimedes where you can put in real data from a real patient on all these variables. If you change one variable you can see what the results will be. It is not about achieving an arbitrary threshold; it’s about achieving better predictability.
The data is fed in and then you get a print-out. They get comparisons not only of national stats but also to their peers. They can see how it progresses.
There are 3 practices here who made no progress. Why? One of them lost their physician champion. One tried to introduce an electronic health record and got sidetracked. A couple made a little bit of progress. But from here there’s a breakpoint. Some of these went to over 20 measures in getting feedback.
Outside of IPIP, there are groups who use national benchmarks. Here is a real-life example where the shift from the old to the new is actually taking place. There are now practices in many other states. Two and a half years into the project there will be over 300 practices. There is now sufficient data to show significant improvement. It took 8 months to begin to see results. If you’re going to ask for physicians to collaborate with other practices they have to know it is going to take time to make improvements.
Q: Is there financial support for this?
A: Yes, it is mostly in-kind. Colorado has received over $7m towards this initiative. This is done mainly by the payers.
This is terrific. There is a loop between the pre- and the post. We first have to acknowledge that the gap is there. This is what we are describing here in our need for continuing education.
This is remarkable and I applaud the project. It’s important to find out how this group can take advantage of the relationships we already have. Maybe we can go to NC or CO and talk to the coalitions about the GMP? We could ask them how it would be useful to them. This is a good example of leadership and how we can tap into what’s already on the ground for this agenda.
Q: Where do the coaches come from?
A: They come from the QIO. They’re full time and adopt a series of practices. There are going to be more. There is probably 1 QI coach for 6 practices.
Q: Have you explored the opportunity of including medical students in this project?
A: It hasn’t come up. Thank you for the suggestion.
I’m part of the Dartmouth co-op and the coaches are paid for by the grants. There are also other things happening along this line. Medicare is doing this. You can sign up for getting this feedback which really makes a difference in improving your practice.
We also have a similar program. There is a powerful effect if your practice is listed publicly like this. If you’re near the bottom of the list the first year, you definitely don’t want to be there the second year.
We have to find ways to use infrastructure for more widespread success. The physicians would prefer to see data appear as opposed to having to enter it. It would be good to consider things like that. It would be good to use something like the eFolio to gather this data. This is a very fertile area for us to explore.
There are places that have a CAP program which has been released for use by doctors.
HR Staffing
http://nationalalliance.pbwiki.com/na2:+Human+Resources+to+Support+Alliance
 The Alliance is in a transition phase and we have to consider the resources and skill-sets that we need to make it. We need to pursue additional grant money, have a webmaster, a summit coordinator, a project/pilot manager, an event planner, and a CFO.
The Alliance is in a transition phase and we have to consider the resources and skill-sets that we need to make it. We need to pursue additional grant money, have a webmaster, a summit coordinator, a project/pilot manager, an event planner, and a CFO.
We talked about the articles of confederation and we thought that was a good way to proceed. We identified some needs in the transition for a structure which would have someone who is responsible for "managing" staff resources, maybe 5 members who volunteer as a steering group, then draw names/with staggered terms, have rotating two members off each year. We could cycle through the participant list and have monthly conference calls as needed. This group would be different from the summit design group. This group assures "work" and communication is progressing between summits.
We come full circle by figuring out ways to fund this.
Q: Would there be an annual budget and who would it be presented to?
A: We thought we weren’t ready to be that structured. As a confederation we need to rely on volunteers.
Q: Do we keep track of our resources?
A: Yes. We do.
Maybe we need to monitor or regularize this?
The need for transparency is apparent now. We’re at that place in our process to formalize this and to be more transparent.
We’d be happy to share the financial information with anyone. We’ve received anywhere between $1000 and $50k gifts and innumerable in-kind contributions.
One of the vehicles to do that is to ask the steering committee to assign this task to someone. We talked about going to a formal board structure but it felt like we weren’t ready to go that far.
This is the time where we need stability of revenue and staff. We need accountability and predictability. We need to put some energy behind the wheels.
Coming from the perspective of participants, maybe we can define two levels of participation? There is sponsorship as well as working for solutions.
The term sponsors has been used to refer to the group of people helping to design the summits. We'll start calling them something else.
We haven’t made clearly public about the kind of support we’ve received and maybe we should make that more transparent? It can certainly be available to everyone who participates in the alliance.
There is a healthy tension in our group between stability of staffing and stability of funding. How do you get that without more structure? If we want to choose a steering committee, we might be able to do that here?
We might want to pool resources from this group to advance the work in between these meetings? In order to maintain momentum we need to do things between. The steering committee provides a resource to the staff that advances the work.
Americans had a unique ability to proliferate organizations more than any other culture. I think a steering committee is fine, but I think it’s important for the group to consciously decide how much structure we want and need. We need to ensure that those of us who have substantial roles already can come together and convene in a consensual manner. Maybe we could try it as a trial?
Form should follow function. There needs to be a middle ground because this is an iterative process.
One of the things that is a problem is that the funding cycle is very short. Maybe what we need to do is to ask the participating organizations to make longer term pledges? Then they could look at the activities and how much staffing we need. This doesn’t have to be connected to the question of providing leadership to the process. These issues don’t have to be intertwined.
They do intersect because if we ask for additional resources the organizations contributing will expect oversight.
Is there a sense that we want to choose a steering committee?
Sense of the commons says yes.
Let’s call for volunteers.
- Aschenbrener, Carol
- Clark, Danny
- Cohen, Jordan
- Fedor, Robert
- Finelli, Frederick
- Hoven, Ardis
- Little, Brian
The first meeting of the steering committee will be shortly.

Scribing
Click on a thumbnail below to open the full size image in a new window