Introduction and Opening Updates
 John Becher
John Becher
Good morning. I’d like to welcome you to our session. We have some ground rules that I’d like to go over. If you digest these and go with the flow, it will work for all of us.
Ground Rules
|
It is traditional to start off these summits with a poem. Thanks to Carol Aschenbrenner for this one.
Yes by Muriel Rukeyser
Some go local
Some go express
Some can’t wait
To answer Yes.
Some complain
Of strain and stress
Their answer may be
No for Yes.
Some like failure
Some like success
Some like Yes Yes
Yes Yes Yes.
Open your eyes,
Dream but don’t guess.
Your biggest surprise
Comes after Yes.

 Michael Kaufman
Michael Kaufman
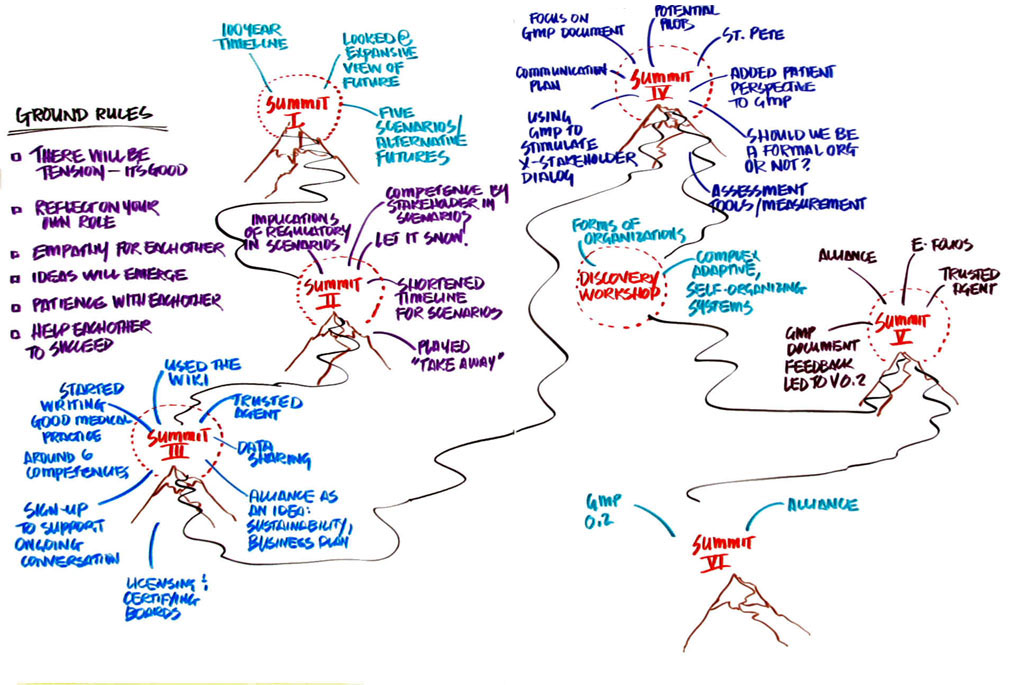
Let’s all take a moment to remember what has happened over the last 3 years. Does anyone remember what we did at the first summit?
We looked at a huge broad picture. We developed a 100-year timeline. We produced five scenarios. Scenario Planning is a tool that Shell Oil developed to help people think about alternative futures based on the most significant and most unpredictable trends and events and where the intersections between them are. This helps people prepare for multiple conditions and be ready for which ever future actually happens.
In the second summit, we took the scenarios and realized that things were moving faster than we initially thought. We looked at the implications of these various scenarios on different stakeholder groups. We explored regulation and what it might look like in the different scenarios. We played a game called Take Away and how the taking away of essential components might influence the way we think about the regulatory system. We looked at how the measurement of competence might change in each of these scenarios.
In the third summit, we started working on the wiki and attempted to create a common language and an outline around a general set of principles of competencies. We also looked at the idea of a trusted agent. Something miraculous happened at that summit. Don got up and asked for people to support the continuation of the effort and people did.
In the fourth one we started looking at the continuum aspect of medical education, training and practice. We had a small group of licensing and certifying folks together exploring ways to align their efforts. We looked at how to create dialogue and changes to the theoretical model. We added the patient perspective to the GMP document. There was a lot of conversation about this thing called an alliance. We talked about assessment as well in this summit.
Then we had a discovery workshop and looked at many disciplines and types of organizations that might be valuable and give us a fresh perspective on how to think about the forming of an alliance.
In summit five, we talked about the alliance, the trusted agent, and the sharing of data. We had three tracks: the emerging alliance, data, and good medical practice. All of this led to 0.2 of the GMP. We had the utility survey and the draft participant agreement as tangible outcomes and used them as inputs for this session.
And now, we’re here.


Opening Updates
What’s happened outside of these summits?
We’re thinking that there are contextual issues with some content. How can we have consistent messages about a person’s career? Before these summits I would have thought about this in silos, but now I’m making phone calls to people I’ve met here.
We’re about to partner with several members of our community to see how the competencies are used.
The eFolio conference was designed by four organizations that come to these meetings. The impetus for this started at the summit in St. Petersburg.
We read Spider and Starfish and when I think about the number of organizations that are represented here; I know there are so many things going on. The kind of relationships that we’ve been able to make here are an incredible outcome already.
We have started to use the individual competencies in our practice and I use it when I talk to professional organizations.
In summit 2, we saw that things were happening faster than we imagined. Are we really seeing a sufficient case for change in the circumstances that support our ideas?
MK: There’s a drive towards outcomes and what those might look like. Do you have something specific?
I’m unclear whether this unstructured process is adequate to the task we have in front of us, and addressing competency.
MK: If you knew where ‘there’ was, do you think we could put that on a timeline?
Legacy systems and our current hierarchical structures are so strong that they are our biggest obstacle.
We may need to use them to get where we want to go.
MK: I call those spheres of influence. Not one of us could change this whole thing, but all of us can affect our spheres of influence to change the system.
Sometimes things aren’t moving fast enough and at other times, when things coalesce things happen very fast when we don’t even realize it.
MK: We need to deal with our own limitations when dealing with emergence. There is some challenge that each one of us has in having less control and letting things emerge as they will. No one is saying ‘you should have this dialogue; sometimes that’s hard for us to manage.
We have two different metaphors going on, both an arrow shooting at a target, and flowers blooming. Maybe the flowers that have already started to spring up would be enough for us to feel that we’re doing enough. If we switch to a metaphor that we’re gong to shoot our target, we take on a completely different feeling. Maybe we just need to see where there are some open spaces and plant some more seeds there to create a richer garden?
The message I’ve taken is that the response is too little too late. The government is now taking the lead. Had they acted more swiftly and gained public trust, they might have had a chance. We can’t lose our sense of urgency.
I don’t view the public as shaking the stick, but in general they don’t focus on what’s wrong with the practice, but what’s wrong with its principles and commitments. We came together because we’re worried that our profession is losing our mores. If we don’t act in a proactive way and take responsibility we’re going to lose the game and the trust.
I think the public is demanding it. I say that the state legislators are taking small steps based on hearing from their constituencies.
I would ask is it not just dissatisfaction in a larger sense, providers, patients, family of patients, nurse practitioners, etc? There is a lack of satisfaction across the board. A lot of well-meaning individuals are suffering in a bad system. The change of status and function in physicians is a fundamental paradigm shift. They didn’t see themselves as captains but as 5 star generals. I don’t think it’s necessarily that it’s just the public distressed by the physicians but them and the physicians distressed by the entire healthcare system. We need to be careful how we frame the discussion.
I wonder if the public expectation has risen too much. I could never meet them given the tools I have. I think we have the wrong end of the stick. Physicians cannot be perfect. I want to be as competent as I can be, but I will never be fully competent.
There has been talk about trying to attain an unattainable vision of competency. It’s frustrating to try to get to a place that we can never get.
MK: This could be resolved by the way we think or talk about this in the system. We’ve talked about whether it’s punitive or aspirational. A man I met on the plane told me about his teaching of police officers. In their final class he asks them if they think their job is about fighting crime and shows them the kind of results they might get if that is what they think their job is. Then shows them that if they considered that their job is about creating peace they would get completely different (better) results. This is what we might be doing here: Reframing the way we think about the entire system.
Maybe our state licensure process should include more people who come from the public and are not necessarily trained physicians? We can look forward to embracing the inclusion of an informed public. Over time, they understand the perspective of the physician and bring a nice point of view.
We don’t have to try to achieve perfection but we can hope to simplify the complexity and map that out on a timeline.
We know that of the mistakes that are made it’s not just that we have incompetent doctors and nurses but most of the time it’s because of a system that has set them up to fail.
What if we changed the title to National Alliance for Health System Competence? We really are in a paradigm shift. We’re talking about a more systematic change.

MK: One of the outcomes that came out of the discovery workshop is we want to create a commons for discussing these difficult issues and it might be time to start including conversations about bigger issues in the system. The initial question that drove all of these summits was ‘how can the physician community determine, measure, and assure the public of physician competence for the life of the physician?' If we don’t self-regulate, then we will be regulated. There is enough bubbling up of the other issues.
The smaller question is physician competency and the tools to measure that and we discover the bigger issues with the healthcare system.
The Board of Surgery is considered as having two stakeholders, the patients and the physicians. It doesn’t have to be a balance as much as a Venn diagram where there is a space for the win-win for both of these groups. We don’t have to choose one side over another.
If we go to an even bigger question, we go beyond our sphere of influence. Maybe we could have a document that explains the conditions for physician competency? This might be an interesting piece to have in one’s pocket.
We’re an emergency oriented society. We’ve designed the summits around this emergency. We’ve come together in a wonderful way to develop a plan which creates a foundation for a good healthcare system. We’ve found a way for people in silos to come together. This is the beginning of a process and articulating a vision of what can be. We can complain about the system but we need to articulate what can be and that’s what we’re doing.
There seems to be a tension in the room between getting our ducks in a row and addressing larger issues. Do we want to get our sphere of influence wider here? Maybe we need to involve the policy makers? Are we going to be in the tent as a profession? If you need urgency, we’ve got January 2009 looming right in front of us.
I got the chance last Friday to hear the Declaration of Independence read out on NPR. What a spectacular document. Maybe we need to come up with something like that? Do we need a Thomas Jefferson that could take the GMP document and make it something worthy of each of the physicians in the room? I think it could be something that all of us would want to live up to.
Physicians are part of the healthcare delivery system. Part of our issue is that we need to become involved at a macro level. If we continue to abdicate this responsibility, the target will keep moving.
MK: Are there other things you know of, other flowers that are growing, that would be valuable for us to know about?
Some organizations are trying to evolve technical staff to have new systems.
There are public members in this room but not many. There are no payers in the room. This is a problem. We need to think about why they need to be in the room. How can they support the profession and know the implications of the profession as we go forward? I would like to reach out with a compelling reason for them to be here.
Physicians are only a small part of providing medical care. The vast majority of care is provided by others, and we need to be cognizant of that.
I have a concern about the generational representation we have here. The people here have grown up with a particular system but younger people have a different idea of where they want to go. I would make a plea to have better representation from the younger generation.
There is a whole area in the GMP about communication and mostly it refers to patient communication, but there is also an importance of the communication between us. Also, I have said this at the third summit and I’ll say it as long as I need to: the kind of people helping the patients are different than the patients they’re helping and we need to change that.
The biggest frustration is that some doctors out there are just assholes. They need to communicate differently. As soon as someone let’s their professionalism lapse, I will not advocate for them. We should hold standards for this profession, but the level of specificity is sometimes outside our sphere of influence. Let’s set our sites the right way.
There is a movement going on which is the patient-centered group demonstration. Most of the 100 members are not of the medical profession. This is looking at putting the patient at the center of their own medical care. They’re re-defining competence as a state that the physician is in against a process of healthcare. Some people feel uncomfortable about a state of competence that the physician can achieve.
There is a great patient safety movement going on focused on compassionate healthcare who also know that physicians are humans and not perfect. We don’t want regulation; people are just demanding that things are better. I was cited in an article about this in Reader’s Digest and I’ve already received 600 phone calls about it. The public is getting excited about this and taking charge.

Michael Kaufman: I just want to remind you how we work. You’re going to go out to small groups, get an assignment, work on it in a collaborative way, and create a product and come together to share what you’ve done.
There are no formal breaks, so if you need to get up, please take care of yourself and be sensitive to your environment.
In each round of work every group will have to make a poster, document into the wiki, and create a video.


Scribing
Click on a thumbnail below to open the full size image in a new window