Closing

Let’s start with having a representative from each track talk about the accomplishments of each track.
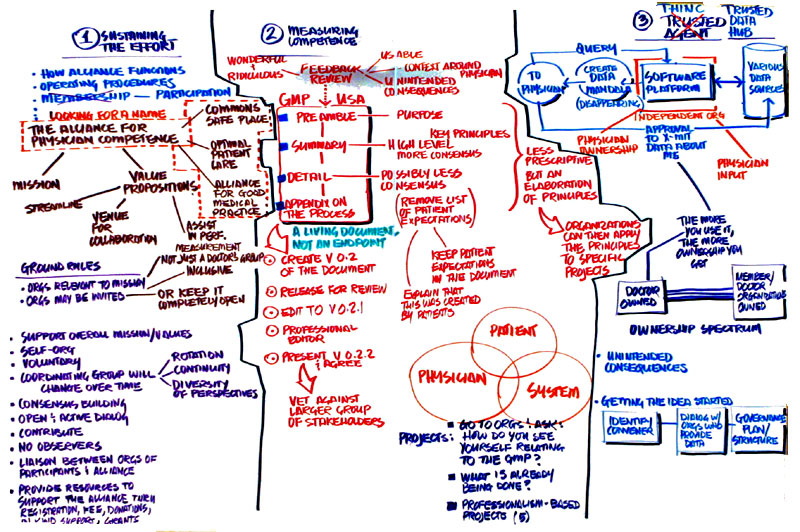
Track 1: Sustaining the Effort
We discussed the nuts and bolts of how this organization functions, its operating procedures and processes.
We first discussed a name. If we’re going to communicate effectively, we need to have a good name that will last for a long time. We developed a mission statement. We developed value propositions. We’re going to provide a venue for collaborations among the various organizations. We will assist the medical profession in physician performance measurement.
We had a discussion of the common ground rules that we’ll operate within so that we have a common shared idea of where we’re going together. It’s important that we don’t call this an agreement or a membership. This is a voluntary activity so we stress the world participation. Any organization with a core commitment to the mission can participate. We consciously discussed that there shouldn’t be groups that come in and be disruptive. The alliance moves into a more careful arena where relevant organizations will be invited to join instead of being completely open.
Before becoming active in the alliance, the organization must agree to various principles, such as acknowledge the self-organizing nature of the alliance. The leadership will change over time as the needs change. The leadership is the coordinating group and not a voting group by any means. They will need to commit to the framework of consensus building. They will agree to regularly attend meetings and offer constructive input. The process will not accommodate observer status.
The final point is how we’re going to facilitate and fund this will be through registration fees that will help finance the meetings, in-kind support and donations. The donation size will not be based on any criteria but rather what the organization thinks it should donate.
There is still a lot of discussion on the name of this thing.
There are many components to the financial considerations. There are opportunities to go out for grant monies. It would be part of the responsibility of the coordinator to go after these funds. The human resources function is to have a coordinator and we need a staffing model. We would have the program coordinator who is housed in one of the organizations, such as the FSMB, where it started. The salary of that person would be subsidized through the other organizations that are part of the alliance and the position would be responsible to the alliance. There are other opportunities to staff in kind resources. Being able to tap into the resources from other organizations will be essential for continuing our efforts.
The sponsor group would be self-sustaining and would select replacement people from the larger group. They could be identified from a participating organization based on a list of skills. It needs to not be seen as a club, but the best assembly of resources from amidst the group. No one organization should have more than one person at a time. The diversity is really important.
I have a question for the group. I’d like to change the group composition to be more open. What do you think of that?
I think the group will be self-select anyway.
One line of thought is that we avoid the names of physician, alliance, and competence but something like leapfrogger.
I wonder what are the selection criteria. Is there an open-ended way of doing this? There is something appealing about this being an open organization. I agree with not having a membership structure. Even ‘alliance’ sounds clubby. I wonder if we’re trying to solve a problem that isn’t a problem. I like the sense of non-exclusivity.
I like the concept of a commons. Trying to say that people can’t use the commons or finding a name seems premature. The name might limit where we go. I think it’s too early to do that.
I’d like to speak in defense of the word alliance because it indicates responsibility. What we need is to have organizations to step up and say yes, we take responsibility for this.
We’ve gotten through some tough points through the diversification. I think we run the risk of becoming myopic in our thinking
There was an old radio program called The Shadow, “what evil lurks in the hearts of men”. When we say we don’t take lurkers and invite non-lurkers, are we getting to where we want to go? What you need is a process that identifies how to get past the evil in our hearts and bring the whole person there.
I’d like to see a vote on having a coordinator to move this work forward and are willing to provide funding to make this happen. Almost all of the hands.
  
top of page
Track 2: Measuring Competence
We addressed the document at gmp-usa.com. We reviewed the feedback that was given in advance of this meeting. There was a wide range of responses from wonderful to ridiculous. We know it needs re-writes and some more work. We considered whether it should be more than one document. We looked at the overall thing and arrived at consensus to add a preamble and then a summary document which highlights the principles. These come from the ACGME and are universally agreed upon. There is another section which would have the detail. There is less consensus surrounding it but a general sense of value and it has an aspirational quality. The details would be clearly described as something we’re striving for. Then we would have an appendix with the process, details, and copyright stuff that has to be in there.
We proposed a process to take this forward, not to be exclusionary but to be efficient, so we propose to take the group that worked on it here and put up a strawman 0.2 document that people could work on it in workable chunks. We could then take the large body of feedback for editorial revisions to a larger body. From here we could have a professional editor and legal advisor to polish. Then we would vet that back with the larger body. Once there is buy-in on that, we could possibly consider taking it to a much broader audience as was suggested earlier today.
There are two pages on patient expectations for physicians that we unanimously deleted from the document because it seems past our scope. The doctors shouldn’t describe what the patients should expect. This should be presented as what doctors will hold themselves to. The patients can describe what they expect in a different forum and maybe these groups could come together at some point.
There are variations on how organizations use this. It should be edited by people who are experts in this field. One of the reasons to have public representation is because this document should be readable by non-physicians.
It concerns me hearing that this represent the doctors’ group. There has been a big effort to have it be a more diverse group than that. It may be the perception because of the Physicians Assuring Physicians Competence. I think we’ve worked hard to make this not a doctor’s group.
We had considerable discussion and even though some of us didn’t really want it to come out philosophically, it was hard to go against some of the ideas for taking it out. Initially it was about patient collaboration, and we can be clear about what it is. This is called the Good Medical Practice document and doesn’t have the Physician Competency name in it.
To work with consumer patient group to find extraordinary educational opportunities is essential.
Apart from the content, if this document is supposed to be a guidance, standards, aspirations for physicians, then having a patient’s perspective is not vetted enough. This is a specific subset that deserves its own effort. We need to make a concerted effort to know what the expectations of patients are. We debated having it as a separate document. This would be circulated widely. There were some views that we should keep the documents together.
I’m struck with the idea of the Good Medical Practice document will be used by the professionals in the field or maybe it will be used beyond that.
You can’t practice medicine without patients.
Using that argument, why don’t then we have expectations of payors and health systems, maybe we should take them into account. The inclusion of a patient expectation to the exclusion of all the others is paternalistic. Now we’re taking on what a whole group expects. We should be informed of them and that should affect the document, but I feel uncomfortable with saying that we know what patients expect.
Given that we spent a good part of the afternoon and this morning talking about the document why don’t we name the group the Alliance for Good Medical Practice. That would take care of the various sides.
This group which includes multiple stakeholders has never said ‘let’s tell doctors how to act’. It was to align expectations. This may look like a document for physicians but that wasn’t how it started.
There’s clearly not consensus on this so let’s preserve this conversation and take it to the next process. There is not a desire to exclude a patient and we don’t need to take it out just because that section doesn’t look like the others. The question of authorship will be come into play. This is a loosely aggregated collection of individuals who have put this together.
I want to speak about the process. I urge us to not be perfectionist about this. This is one version and we need to treat it as a living document instead of something we have to get right. I would hate to see us go into having an expert decide how this needs to look.
I got stuck on the words ‘physician’s alliance’. Maybe we need to engage more broadly in this group.
The original summits came up for the idea of physician accountability for physician competence. The idea and name of the national alliance came up in one of the sessions.
Let’s have a straw vote about who thinks the patient perspective on expectations should be in this document. Most of the group.
I think the patients’ piece could be quite an education. This is really an effort to insure the mission to come true. This is not about telling patients what they should do. It involves lots of competent people.
Communication Plan
We did the communication plan. This is a good medical practice document and can’t take place without the patient, the physician or the system. We looked at expectations around all of these things. I love to hear feedback from all the groups to each other. We also need to do a system strategy to figure out who we need to get feedback from. We will have to ask them to review it from various levels.
Pilot Group
We were the pilot project and we’d like to ask the groups how you see yourselves in the GMP. We also did an inventory of things that are being done. We looked at some of the examples of competency and the collaboration that is occurring. There are some things being done in Canada around the physicians’ achievement review. The other areas we spent time talking about were the medical schools, disciplinary actions at the medical schools and ways to look at professionalism and setting standards. We had specific projects that we can suggest.
 
top of page
 Track 3: Infrastructure for Information Exchange Track 3: Infrastructure for Information Exchange
The trusted agent is providing an intelligent cluster of data that is professionally requested. We stopped looking at the workings of the engine to get to the process. We felt very strongly about several things. We didn’t really like the term trusted agent and focused more on the idea of a hub. If there is some type of company that would work around the hub, the Trusted Hub Inc
Having physician input and ownership is the only way this would work. This hub would be owned by the member organizations. This has many favorable points to it but it leaves the doctors out. A doctor ownership model is also untenable. As the doctor uses the system, he gets equity. The hub will always be a choice. Doctors can always get their information the old way.
We understand that this allows the process to be competitive and other better models will emerge. This takes control away from the member organizations. We spent a lot of time envisioning problems, unintended consequences, unanticipated benefits and those were myriad. The tsunami quickly came. Can you imagine having requests from 40 patients and the payors and the rest? This quickly becomes overwhelming. We don’t want to create another burden for the physicians or another level of bureaucracy. We’re concerned also about that we throw a party and no one comes.
We talked about how to get this started. It’s obviously complicated. We need to have a convener, someone who’s willing to take charge. We didn’t agree on a way to develop it. We understand that government input is key. It’s going to be difficult to get into a government structure.
We used the assumption that the alliance didn’t exist when we considered who could get this started. We tried to come up with a name. There were glaring conflicts of interest. We drew names out of the hat to see if they’d be willing to get the organizations around the table to see if they’d be willing to get together. This was one of the most difficult parts of the process. How do we go forward from here?
We left the process thinking this is valuable, but I was overwhelmed by the complexity.
On the other side of the white screen we were doing planning issues and one of the concepts that we developed after we informed everyone about this would be to communicate to the ones who would have to provide the data. We would have to do a gap analysis and find out if they’d be willing to participate.
It’s not that there have been no conversations already around these organizations, but how to pull it together as a viable working model is the next step. Because the Federation and the National Aboard have been more involved, it would be helpful to have another group be the convener. It’s better that it’s not somebody’s plan.
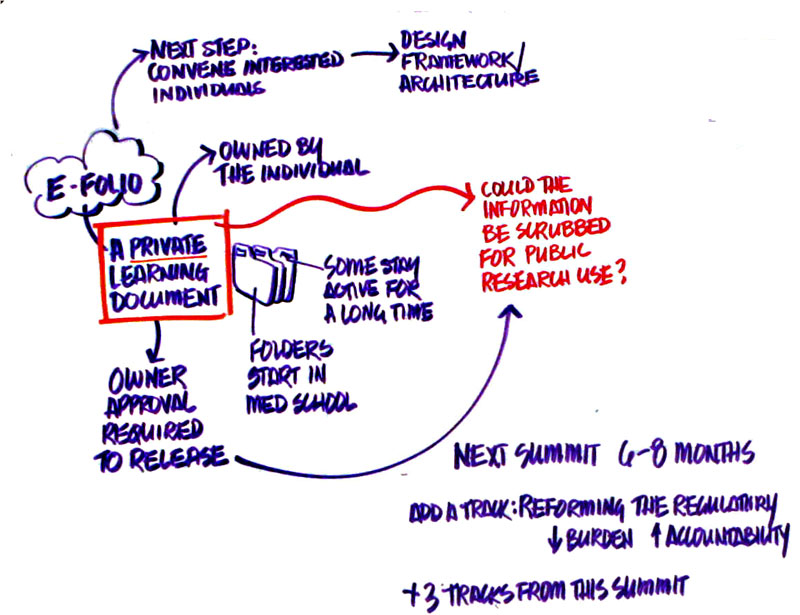
 eFolio eFolio
We have two groups working on the eFolio who came up with the same conclusions. The eFolio should be considered as a private learning environment. It should not be thought of as having a public and private component, but that it is all private. The eFolio would be things that I gather about my own learning as well as copies of my important documents. The folders would probably start in medical school, maybe even before. Some folders would be archives and others would continue to build over the lifetime of the physician. There would need to be system capabilities to make this happen. We would have a fairly simple structure, though it likely is a very complex technical feat.
We didn’t talk about an action plan but I think we have an outline so that we could keep going on the conversation. We could get interested parties together to come to consensus on the guiding principles and to seek out the vendors to make it happen.
The issue of private vs. public is raised about the ownership as well as a mine for research. That was balanced against the ability of the individual to place negative information in there. We wondered if there would be a compromise. This has to be individually controlled for the individual to use it as a learning tool. We didn’t get to a plan because we would need standards for how to make any part of it public.
It’s just like our email. Everybody has access to their own and everybody has their own kinds of folders.
Sometimes you don’t know what negative is. Sometimes findings are just important. We can use the research database as points of leverage so that we can be more effective.
If within the private learning environment there can be disidentified data that would submitted only by the consent of the physician.
Closing Comments
The next summit will be in the next 6 to 8 months. Someone has to go through all the work of all the groups to figure out what the program will be.
Scribing (click on an image below to see a larger version in a new window)
 David Leach David Leach
This idea of optimism and hopefulness has come through. We are hopeful. We have looked at the facts straight on. You’ve had a lot of interesting questions and I feel inadequate to answer these questions so I offer this
Sands of the Well
Just when you seem to yourself
nothing but a flimsy web
of questions, you are given
the questions of others to hold
in the emptiness of your hands,
songbird eggs that can still hatch
if you keep them warm....
You are given the questions of others
as if they were answers
to all you ask. Yes, perhaps
this gift is your answer.
Denise Levertov |
top of page |
