Presentations - Trusted Agent & eFolio

 Trusted Agent – Bob Galbraith Trusted Agent – Bob Galbraith
Click here to download this presentation
I want to acknowledge my appreciation for all the feedback, comments and appropriate scorn to this presentation. (laughter)
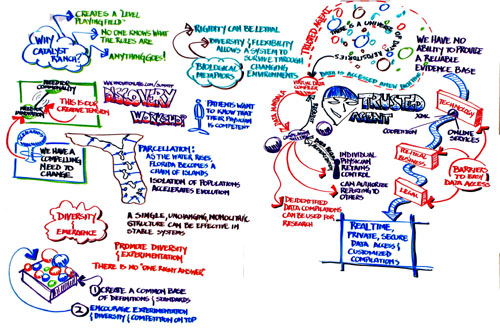
There is a galaxy of repositories of information and all the organizations are separate. The result of all this is that we have an inability to compile an evidence base to support lifelong learning, self-improvement, program evaluation or professional self-regulation.
What we need here is the ability and willingness to share data massively and in real time. We should acknowledge a number of barriers. We have legacy systems, poor operating and data storage systems. There are also political and business issues as well as legal issues.
There are plenty of people who say this is not possible, but I don’t think that is true. I think on the technical level, things have already been solved. The first step is to understand that the bits and pieces are scattered all over the map but maybe we can bring them together through a virtual repository. How do we share data across the repository? That’s where the trusted agent comes in.
I have a slide here of the infrastructure. There is a hub that interfaces between the user who wants information and the repository of data. We have pieces of code which compiles data in order to make it useful to the user. There is no compilation without a user from the medical profession asking for it. You can ask for it to be sent out to other users.
Here is an image of a sand mandala. As soon as it is finished it is ritually expunged. This is significant to our work here. We have data mandalas for individuals. We compile and report to the individuals and then it is expunged from systems after reporting. You can recreate it at any moment. This is essential because we don’t need any “super” new repositories. There is no new discoverable data in the trusted agent because it is expunged.
One of the services you can provide is to give reports to other systems. If you group the data so that it is no longer identifiable by the person, then we can use it for research.
It has to be trusted because it has access to everything all the time. With it online you can have access to it 24/7. It will never compile or report a data mandala unless it has been authorized properly.
 An example of how it works in regard to providing regulatory requirements is this: here is a medical professional who needs to get an application for a common license and requests the information through the trusted agent to pull the information and then can submit it to the right agencies. Anyone who has done this with paper and pencil knows what a nasty task this is. With the trusted agent it is possible to do near real time. Most of the form can be populated with all the information already available and that is already verified. An example of how it works in regard to providing regulatory requirements is this: here is a medical professional who needs to get an application for a common license and requests the information through the trusted agent to pull the information and then can submit it to the right agencies. Anyone who has done this with paper and pencil knows what a nasty task this is. With the trusted agent it is possible to do near real time. Most of the form can be populated with all the information already available and that is already verified.
The CLAF is a pilot that has been operating and to date the record shows that the shortest time to complete the process is 8 minutes.
There was a huge resistance to translating the Bible into English, which is where this picture came from. William Tyndale went to Germany and had it translated there, printed it and brought it back to England.
The trusted agent concept seems like the right answer, but there are plenty of people who are out there who are skeptical. I don’t think anything as bad as this picture shows will happen
Q: I think the concept is fantastic, but I’d like to go back to wikipedia. Trust has two meanings. One of them is the financial one. I think there is an elephant in the room. Many of our organizations’ livelihoods depend on the ability to charge for this information. If this hub reduces their ability to charge again and again for this and their funding sources are threatened how eager will they be to jump on this idea?
A: That’s why we’re not talking about having a super repository. Maybe we could have a different model, such as a membership model with fees. Making sure that the primary repositories maintain their revenue will be key to get them to participate.
Comment: People are becoming more leery of data becoming available. I think we need to have a process that goes both ways.
Q: I’m intrigued by the idea of de-identifying the data in order to use it for research, but I don’t see how that comes and goes. Maybe you could explain further.
A: There are ways to do that. I can describe them briefly here.
Scribing
top of page
 e-Folios - Carol Aschenbrener e-Folios - Carol Aschenbrener
Click here to download this presentation
If you look at the definition of portfolios, you’ll find this in Webster:
- a flat, portable case for carrying loose papers, drawings, etc.
- such a case for carrying documents of a government department.
- the total holdings of the securities, commercial paper, etc., of a financial institution or private investor.
- the office or post of a minister of state or member of a cabinet.
|
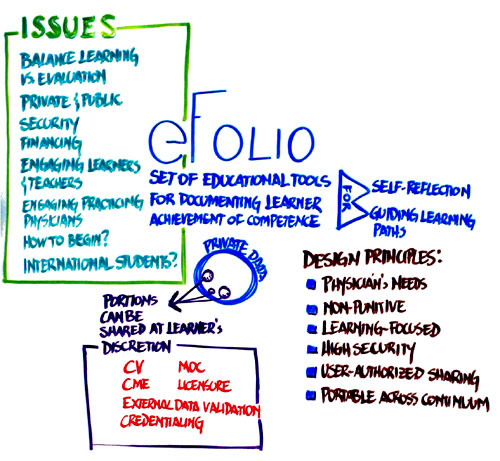
There is a private portion, either entered by the physician or received by the physician. An example might be data that shows continued improvement and that documents CMEs.
At the last summit, we had some conversations about portfolios and about the ongoing efforts, such as the ACGME’s efforts. There are several others. There are bits and pieces and our conclusions is that we will shoot ourselves in the foot by creating a system that doesn’t talk to each other.
To deal with that we had some conversations in May and had 10 experts who are doing a lot of work on these. They wrote a white paper on the state of the art work that is being done. We had about 60 people at that conference who are working on eFolios.
Most of the capabilities here are designed to serve the learner but also to give information to the public. We need to have public consensus. It will need to have state of the art security and confidentiality.
As Bob mentioned, with the credential part of it, it would be the individual physician who would decide how to control access to this. We talked about the various services and functions of the eFolio. Physicians would be able to do self-assessment, mentoring, planning for self-improvement. We wouldn’t keep things in there forever and we would need to decide how we expunge data.
Some of the elements you would want to release under permission. You’d want to share credentials, record of CME, documentation of clinical privileges. This might be used for program evaluation or application.
As we talk about implementing a national system, we see that portfolios are used usually for learning but we want to use them also for evaluation. We need to deal with those two structural layers. We need to protect the private layers. We need to manage the transitions of them when the physician graduates. What will we do with them? We need to define principles around this. If there is a national infrastructure, someone needs to buy into this.
Another challenge is preparing both the learner and the teacher. The learner is the easy part; they’re more techno-savvy and some of them have been in schools that use this. We need an infrastructure to assist practicing physicians to use the eFolio. We also need to deal with the international physicians who come into the system.
We have a number of hopes for the eFolios. This could be a key component that will connect the various agencies. This could be lifetime documentation that helps manage longitudinal information so that we become better at predicting success.
Q: I’m struck with the similarity with the patient’s portfolio. There is a lot of controversy around who owns the record. Most people say it’s the patient, but there are still issues. How can we use this eFolio in a shared way?
A: That’s an important issue. For me that touches on the distinction of the eFolio as a learning tool and it may be used for evaluation. It would be used like the USMLE scores. Those wouldn’t be in the individuals’ portfolio. This would be more for the supervisors. If we want physicians to be free to beef up their learning, that has to happen in a confidential way.
Comment: I think the physician’s portfolio is very different than a patient’s record.
Q: In both discussions, in the context of self-regulation, I think there has to be some balance between self and government. I don’t think regulation is such a bad word. There is a lot more in there than pride. When this comes out into the real world, it doesn’t make sense. Look at Medicare. It’s not helpful. There are some things that should be made available to the public.
Scribing
top of page |
